Appendix
By: Mohamed Hamed MD, Jonathan Kahan MD
Chapter 1: Smoking interventions, the specifics
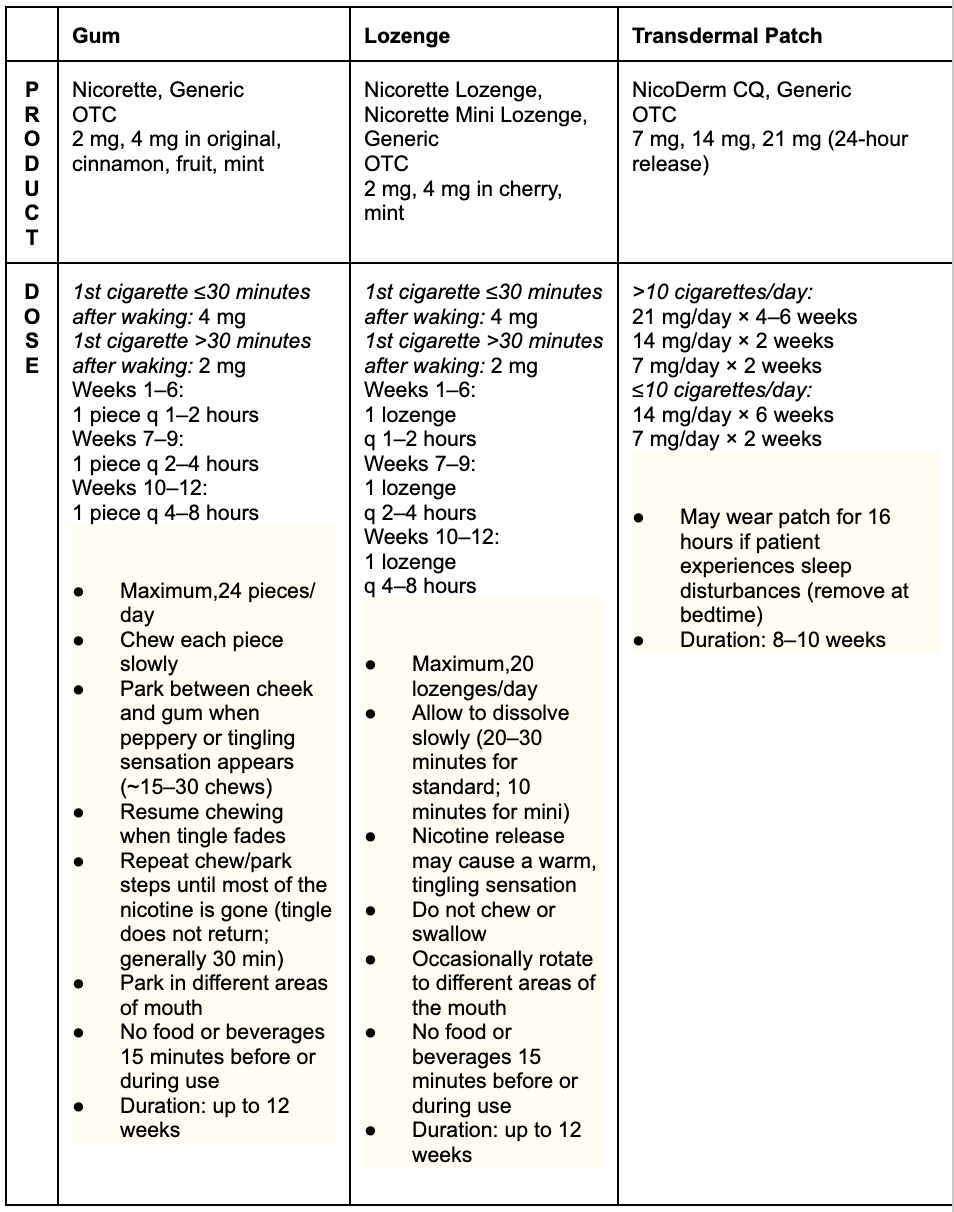
Table 1: Nicotine Replacement Therapy (NRT) Formulations [6, smoking chapter]
Chapter 3: The Lipid pathway expanded:
How cholesterol/triglycerides are processed in the body:
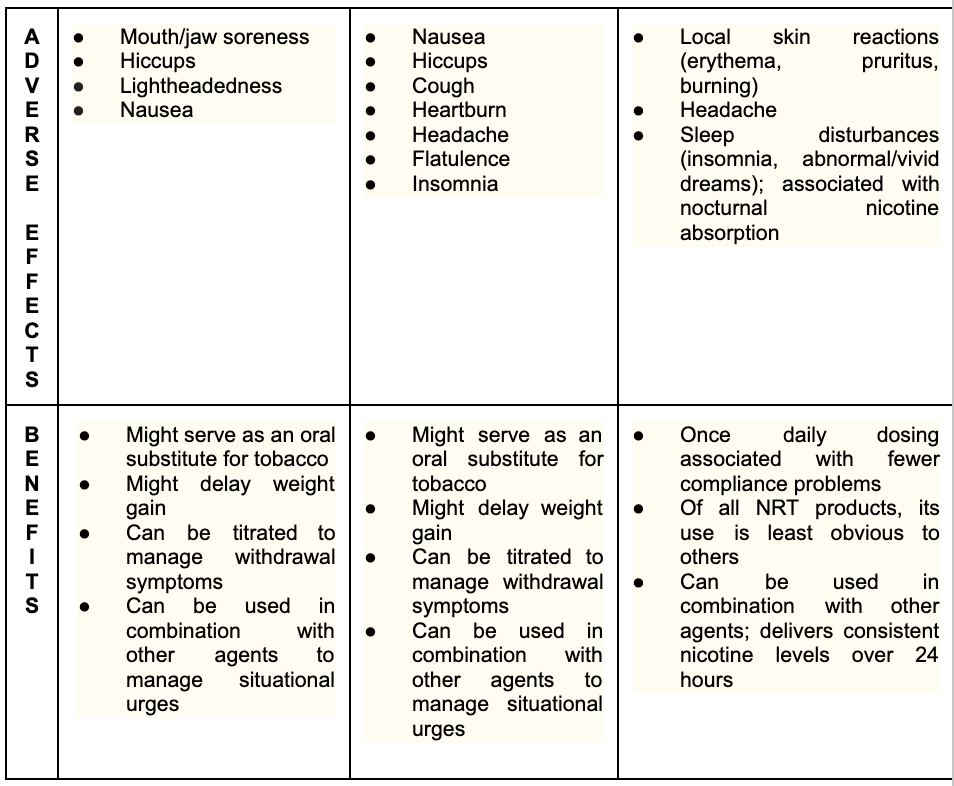
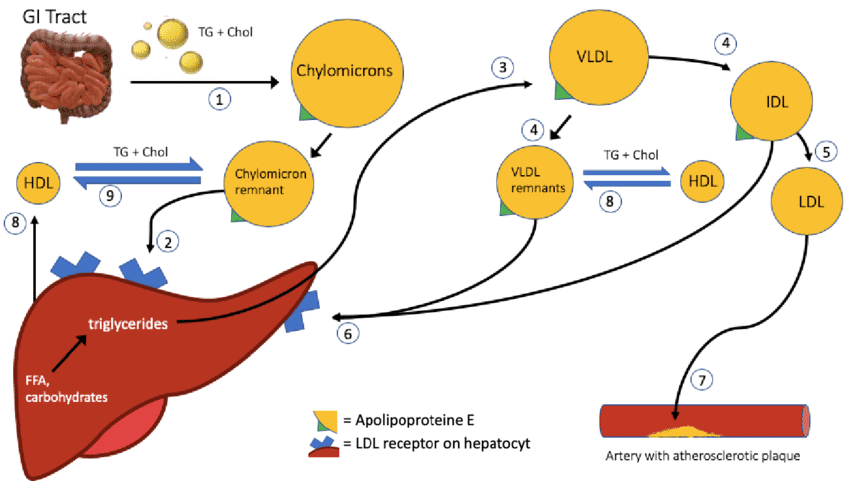
Cholesterol and triglycerides enter our bodies by eating food. In terms of mass, triglycerides outweigh cholesterol 10-100x in animal products. Note plants do not have cholesterol but do have triglycerides. We can also make cholesterol and make triglycerides from excess sugar/carbohydrate intake in the liver.
Triglycerides are further classified into monounsaturated (aka omega 9), polyunsaturated (omega 3,6), saturated, or trans fats. These, and cholesterols, are broken down by stomach acids into smaller droplets called emulsified fats where they travel to the small intestine.
In the small intestine, bile acids from the liver surround the emulsified fat droplets. Triglycerides (TGs) have an extra step and are further broken down into fatty acids and monoglycerides by the pancreatic enzyme lipase (-ase always denotes an enzyme which is a protein that performs a chemical reaction).
These components are then repackaged across the small intestine into spheres of triglycerides/cholesterols within an apolipoprotein (protein) cage called a chylomicron. Once formed, the chylomicron goes from the small intestine cells into the lymphatic system then it gets dumped via the thoracic duct into the bloodstream.
From there the chylomicrons go down the bloodstream into the tiny capillaries that are beside muscle and adipose (fat) cells. A receptor called Lipoprotein Lipase (LPL) takes up the free fatty acids (from TGs) to be used in energy or storage for later in the case of muscle cells and in the case of fat cells they are recombined with glycerol to form triglycerides again for storage in vacuoles (giant balloons for fat storage).
The result of this offloading of TG is the creation of a chylomicron remnant that contains a lot more cholesterol and a lot less TG. This then goes to the liver where the cholesterol is taken up by the LDL Receptor and Remnant Receptor-1 (note the chylomicron does not have LDL in it, it has undifferentiated cholesterol).
Note the liver can make its own cholesterol and triglycerides.
In the liver, the cholesterols and remaining triglycerides are processed and can become several things:
They can become bile acids which can be used to absorb more cholesterol/triglycerides (see above).
They can become High Density Lipoprotein (HDL) particles, which go to other tissues to bring back cholesterols for repackaging or excretion by the liver. The main protein surrounding this core of liquid cholesterol is apolipoprotein A-I (apoA-I).
They can become Very Low-Density Lipoprotein (VLDL) particles. These are spherical mixtures of cholesterols, TGs and phospholipids all surrounded by apolipoprotein B (apoB). The VLDL particles then go to muscle and adipose cells via the bloodstream where they (again) dump TG into these cells via the LpL receptor (again) and the VLDL becomes an LDL (low density lipoprotein) which is loaded with cholesterol. Note LDL is made in the bloodstream, not liver. The LDL then goes and gives cholesterol to various cells to make cell membranes, steroids etc.
Note also that the same apoB protein surrounds all the LDL, VLDL and IDL (the short lived intermediate between VLDL and LDL particles).
Once the LDL particles have offloaded their TG and cholesterol, they return to the liver where they can become Lp(a) or be reprocessed into a.b. or c.
Lp(a) (lipoprotein “little” a): these small LDL (surrounded by apoB) particles can come back to the liver after giving most of its cholesterol, where an apoa protein tail is attached to the outside of the apoB, making it the most atherogenic particle. This process is entirely genetically driven. See below for a whole section on Lp(a)
Reeg, Susanne. (2020). What is the role of ApoE variants in ischemic stroke and other age-related complex diseases? 10.13140/RG.2.2.23487.79529.
B. How the processing of cholesterol/triglycerides results in plaque formation.
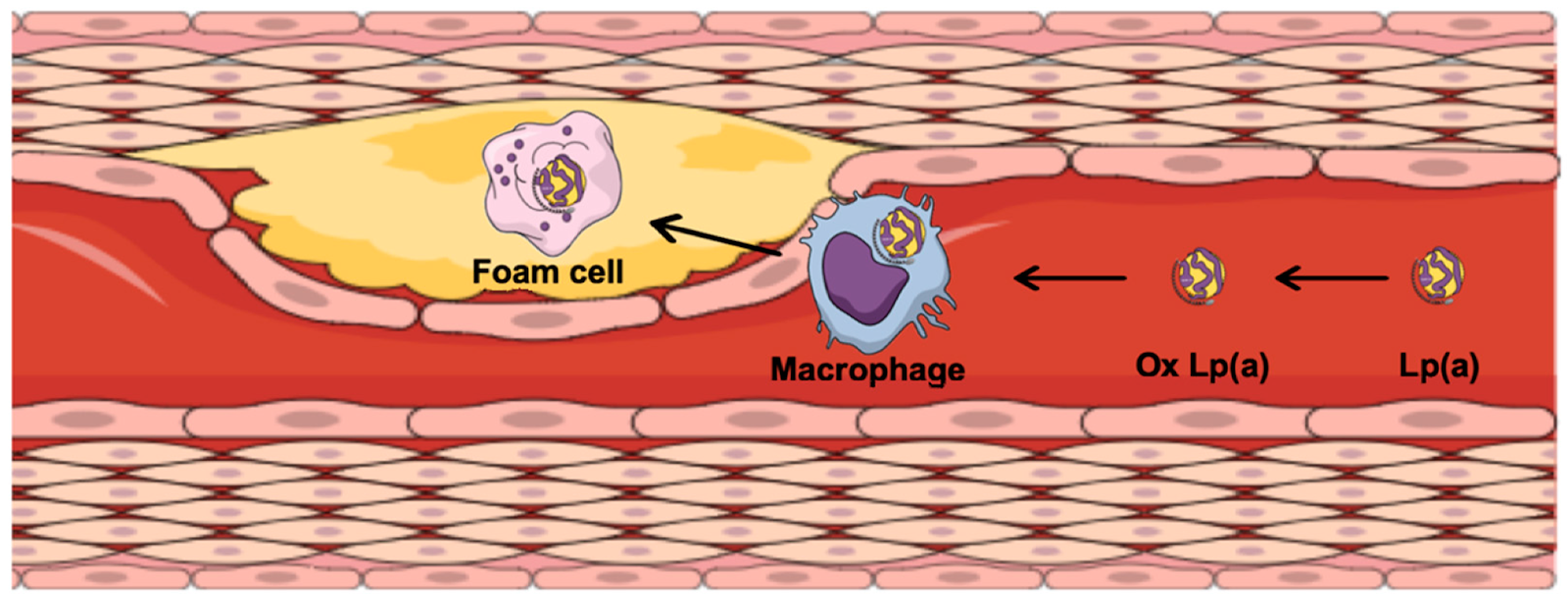
8. The apoB protein (which contains VLDL, IDL, LDL) or Lp(a) (which is the apoB protein, with small amounts of LDL cholesterol and an extra tail) circulate in the bloodstream and become stuck in the walls of the arteries. This triggers a reaction where these particles get oxidized by reactive oxygen species (ROS). ROS can be smoke inhalation, UV exposure, free radicals etc.
9. When apoB or Lp(a) proteins become oxidized the body attacks them with immune cells called macrophages, which eat the oxidized lipid particles and become foam cells, triggering an inflammation cascade and grow to form plaques in the arteries of our body. This process begins when we are about 8 years old!
10. These plaques are unstable and are in the constant process of “exploding and remodeling”. For example, a plaque doesn’t go from 98%, 99% then 100% and a patient has a heart attack, it goes from 20-30%, then to 70%, then back down to 60%, then 100% and a patient grabs his chest while having a myocardial infarction.
11. We are done! Jeez!
Ugovšek S, Šebeštjen M. Lipoprotein(a)—The Crossroads of Atherosclerosis, Atherothrombosis and Inflammation. Biomolecules. 2022; 12(1):26. https://doi.org/10.3390/biom12010026
C. Not so fast! What about cholesterol synthesis in the liver?
In the liver, cholesterol starts with the production of HGM-CoA, whose creation is halted by the statin class of medications. Once cholesterol is made it is then packaged into the VLDL and then converted into LDL in the bloodstream by the same mechanisms above or converted into bile acids. This whole process is regulated by dietary intake, internal controls, hormones, genetics to ensure the body has adequate supplies of all forms of cholesterol.
Chapter 4: Obesity/Nutrition: List of NOVA Class 4 Foods (to avoid)
Sodas, Energy, Sports and Soft Drinks (both regular and diet). Includes sweetened teas, coffees, fruit drinks.
Packaged Snacks - chips, pretzels, flavored popcorns, snack bars, flavored crackers, other similar snacks
Instant Noodles and Soups - products that require minimal preparation
Confectionery and Sweets - Candy, chocolate, gummy snacks
Packaged Baked goods - Commercially produced breads, cakes, pastries and cookies
Breakfast Cereals - most pre-sweetened and flavored cereals
Processed Meats - hot dogs, sausages, ham, deli meats
Frozen Prepared Meals - TV dinners, frozen pizza and other ready-to-eat meals
Processed Cheese products - cheese slices and spreads with added ingredients
Energy Bars/Meal Replacements - bars and shakes formulated with various additives
Sweetened Yogurts - yogurts with added sugars and flavorings
Instant Desserts - packaged puddings, gelatin desserts, ice creams
Margarine and Spreadable fats - products with additives for flavor/texture
Reconstituted Meat Products - chicken nuggets, fish sticks and other processed meats
Flavored and Sweetened Juices - beverages with added sugars and flavorings
Sauces and Dressings - commercial salad dressings, ketchups, mayonnaise, bbq sauces and other condiments.
Chapter 5: Exercise: PeriodizationLinear Periodization (most popular)
Annual Plan Overview:
Four Times Per Week (alternate upper/lower body): Progressively add 5% weight every month until plateau. Start low and go slow! Alternate higher sets+weight+lower reps every few months for variation (eg. 5 sets x 6 reps x 10% higher weight).
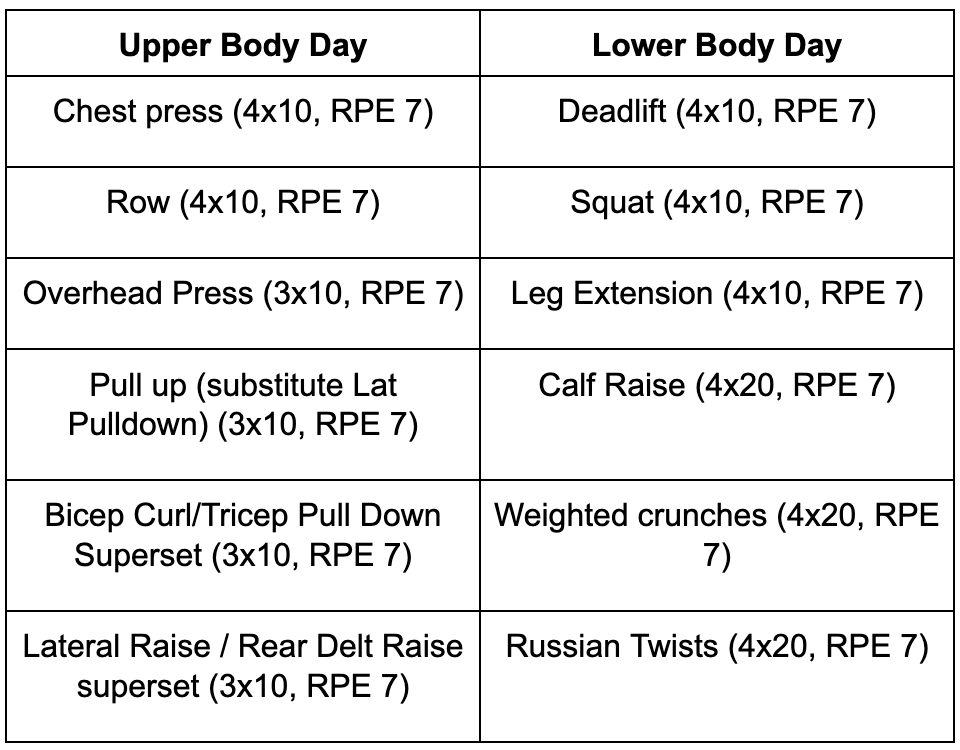
****It is this easy, weightlifting does not have to be complicated!****
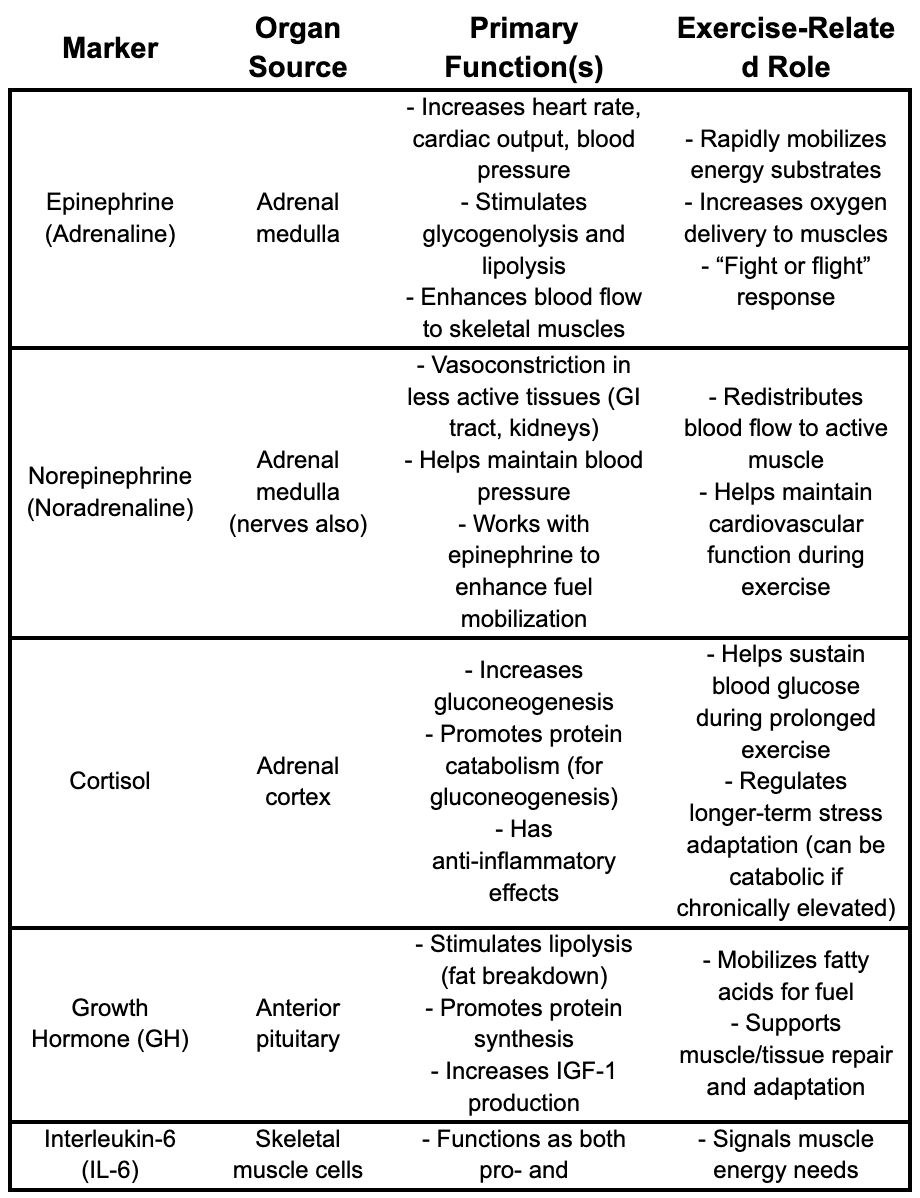
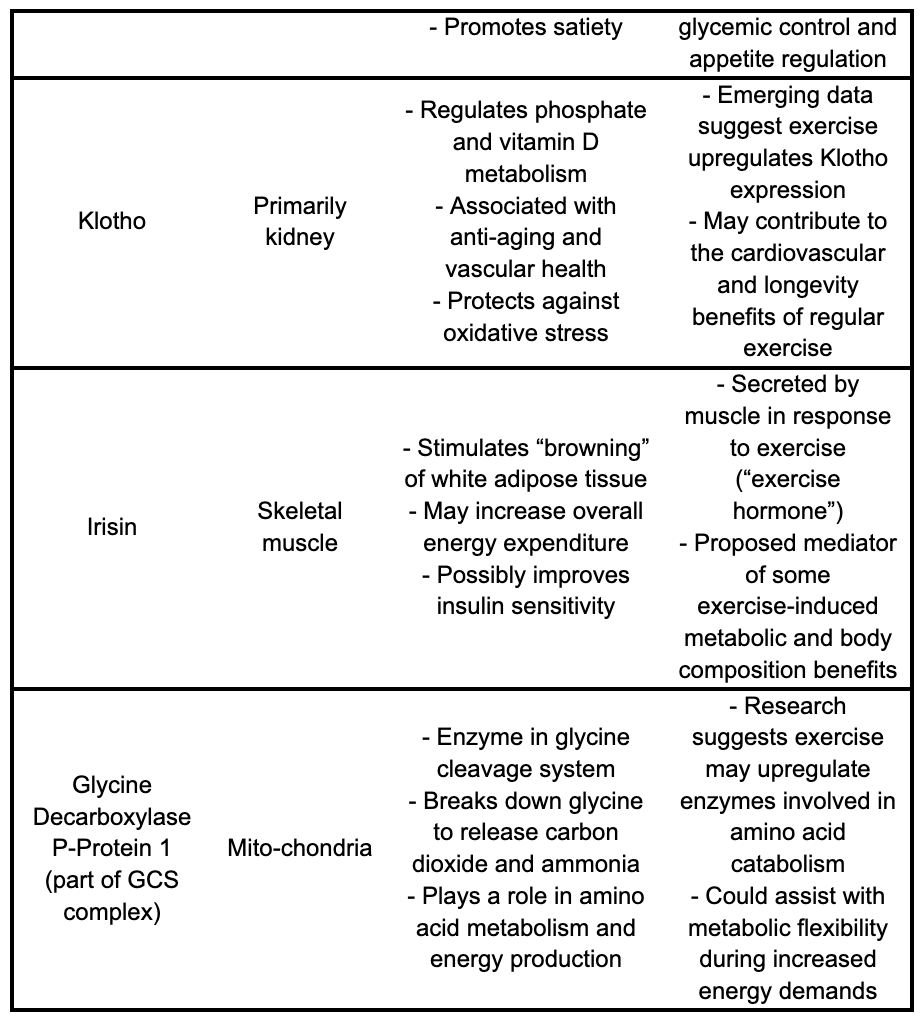
What hormones/body chemicals are changed during exercise and what do they do?
*These are the targets we suspect pharmaceutical companies to pursue in the near future. You will also hear these markers discussed in various medical context.

Chapter 6: Miscellaneous: What labs do we routinely order?
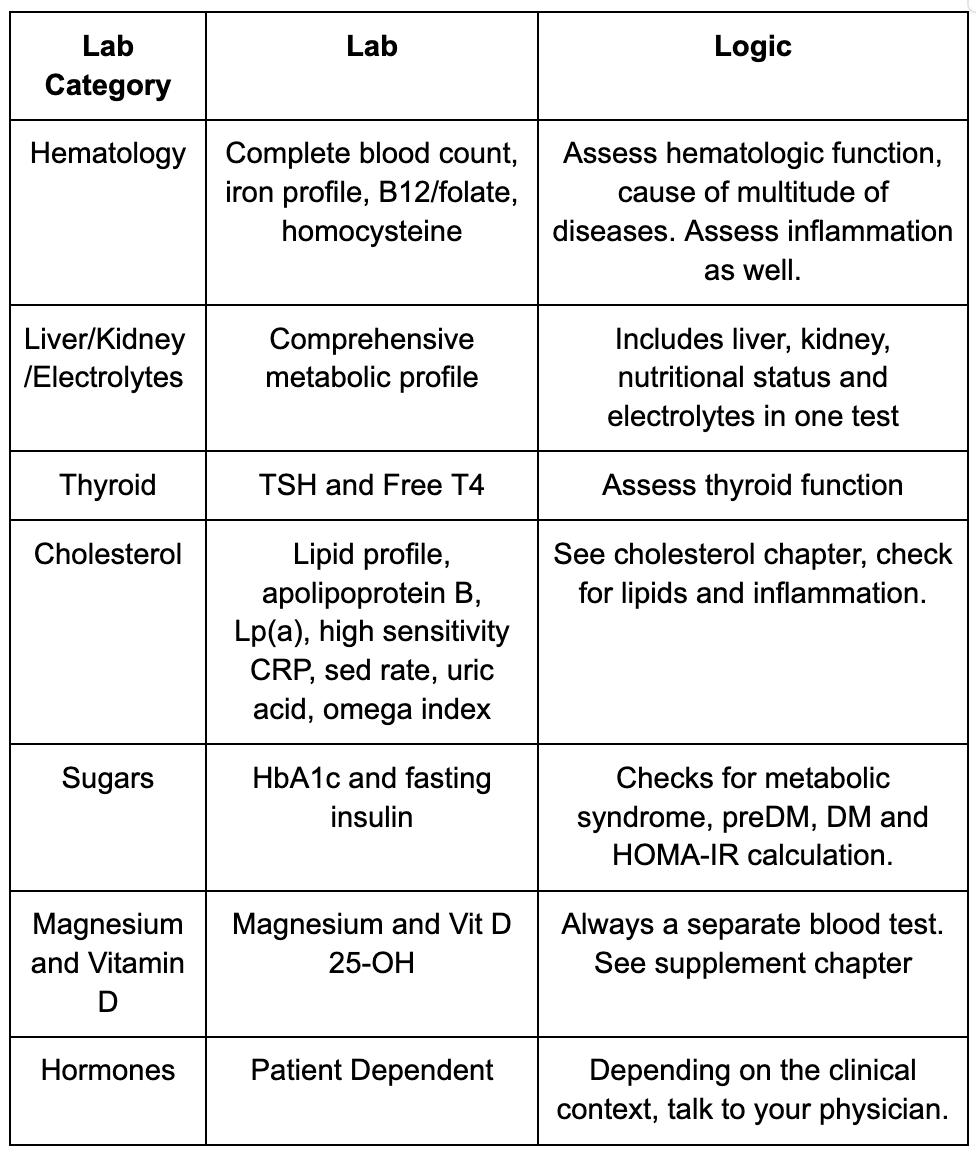
****Note this is not an exhaustive list and is highly patient dependent, talk to your health care provider*****
Practical Approach: A sample routine to get started.
By: Jonathan Kahan MD
This is a comprehensive sample routine, start to finish, on how to lose weight, correct metabolic dysfunction, treat the main causes of heart disease, and immeasurably improve your life.
STEP 1: Gather the Basics
Calculate TDEE ie. your metabolism.
Weigh yourself naked in the morning before anything, start doing this every day, get a scale. Check your height too once. Write down or track weight results over time
Get comprehensive bloodwork routinely, calcium score (every 3 years), get a blood pressure cuff and cross check it with a medical professional, consider a Dexa scan for baseline body composition (not a must).
Write down everything you eat for 2 weeks (brands, sub brands, quantities etc) to identify which foods are processed etc. (move onto step 2 while you complete this).
STEP 2: Set Up Time
Join a gym or get access to weights/resistance training, buy a pair of solid running shoes or cross trainers for support. Consider smart watch to track (not a must)
Evaluate Work environment - most calories burned comes from NEAT, get a treadmill/standing desk, schedule walks/exercise snacks.
Kitchen makeover: Go to your fridge/kitchen and get rid of as much processed food as possible. Buy as much whole foods as you can. Leverage farmers markets, organic sections of large stores, and apps to load up at least 80% of your kitchen with unprocessed foods.
Sleep Hygiene: Get your environment ready (cold, dark, no screens, quiet or white noise, action plan for partner sleep)
Step 3: Intervention
If you are smoking, set a quit date and pick up nicotine replacement
Aggressive treatment of blood pressure and cholesterol. (possibly using medications)
Start exercise routine: weight lifting and cardio eg. M,W,F - total body weights, T/T - base/zone 2 cardio, S - rest day, S - HITT training. Incorporate sports/exercises you enjoy. Go with consistency and effort here, you will see results.
Overhaul diet: experiment with which foods make you feel full, weigh daily to ensure adequate weight loss, adjust what isn’t working, establish a food routine. Work on the 3T’s to leverage a diet, can use Med diet as a framework. Focus on high animal protein and fiber. Avoid alcohol. Find your super foods (Greek yogurt etc) to guard against restaurants/late night snacking. Start meal prepping for work for the week.
Sleep starts in the morning! Follow the 3,2,1 rule of sleep, avoid sleep aids, caffeine only in the AM. aggressively treat snoring/OSA, if wake at night then meditation/box breathing.
Militant cell phone limitations (ie. put it away when home), never sleep with cell phone, meet people in person, get out in nature regularly, look for a higher power (religion, family etc).
Step 4: Re-evaluation: Routinely re-evaluate steps 1-3 on a 3-6 months basis, always have an experiment going, never stop learning.